What is glaucoma?
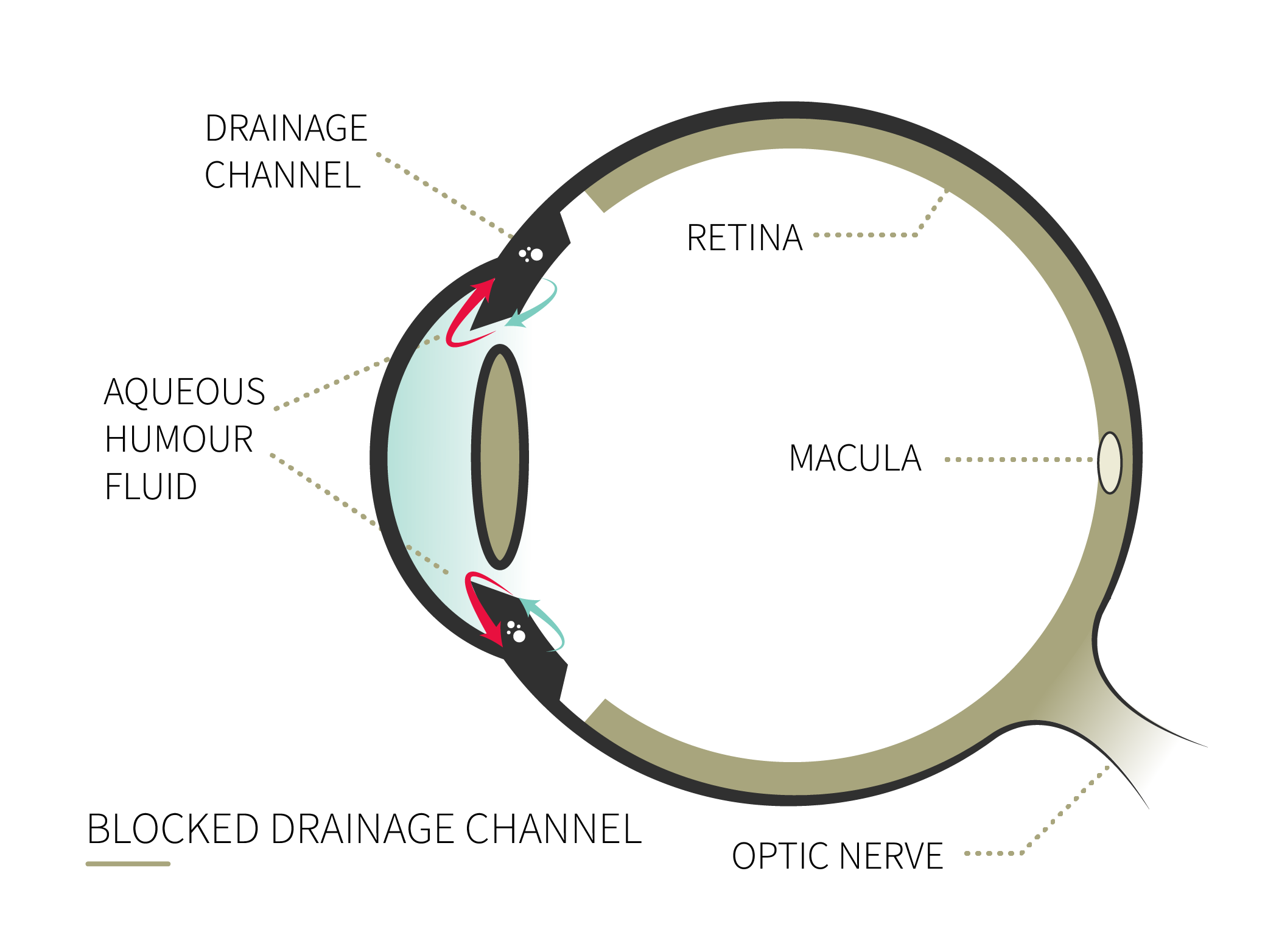
Glaucoma is an optic neuropathy that affects the optic nerve. The condition is often associated with high intraocular pressure, but that is not the only indicator for diagnosis.
The disease includes a series of symptoms whose direct consequence is the degeneration of sensitive eye tissues, retinal nerve fibres, and especially the optic nerve that transmits information to the brain. In most cases this condition is the result of increased intraocular pressure.